Difference between revisions of "IPLab:Lab 3:Tuberculosis"
Seung Park (talk | contribs) (→Journal Articles) |
(→Journal Articles) |
||
| (8 intermediate revisions by 2 users not shown) | |||
| Line 15: | Line 15: | ||
File:IPLab3Tuberculosis5.jpg|This high-power photomicrograph of a tuberculosis granuloma demonstrates acid-fast bacilli (arrows). | File:IPLab3Tuberculosis5.jpg|This high-power photomicrograph of a tuberculosis granuloma demonstrates acid-fast bacilli (arrows). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Lung: Tuberculosis H&E === | ||
| + | <peir-vm>IPLab3Tuberculosis_HE</peir-vm> | ||
| + | |||
| + | === Lung: Tuberculosis AFGT === | ||
| + | <peir-vm>IPLab3Tuberculosis_AFGT</peir-vm> | ||
| + | |||
| + | === Normal Lung === | ||
| + | <peir-vm>UAB-Histology-00107</peir-vm> | ||
== Study Questions == | == Study Questions == | ||
| Line 28: | Line 38: | ||
=== Journal Articles === | === Journal Articles === | ||
* Rodrigues DS, Medeiros EA, Weckx LY, Bonnez W, Salomão R, Kallas EG. [http://www.ncbi.nlm.nih.gov/pubmed/11982602 Immunophenotypic characterization of peripheral T lymphocytes in Mycobacterium tuberculosis infection and disease]. ''Clin Exp Immunol'' 2002 Apr;128(1):149-54. | * Rodrigues DS, Medeiros EA, Weckx LY, Bonnez W, Salomão R, Kallas EG. [http://www.ncbi.nlm.nih.gov/pubmed/11982602 Immunophenotypic characterization of peripheral T lymphocytes in Mycobacterium tuberculosis infection and disease]. ''Clin Exp Immunol'' 2002 Apr;128(1):149-54. | ||
| + | * Horsburgh CR, Barry CE, Lange C. [http://www.nejm.org/doi/full/10.1056/NEJMra1413919 Treatment of Tuberculosis]. ''NEJM'' 2015 Nov 26;373:2149-2160. | ||
=== Images === | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/259-tuberculosis PEIR Digital Library: Tuberculosis] | ||
| + | * [http://library.med.utah.edu/WebPath/LUNGHTML/LUNGIDX.html#4 WebPath: Granulomatous Lung Disease] | ||
| − | + | == Related IPLab Cases == | |
| − | + | * [[IPLab:Lab 1:Tuberculosis|Lab 1: Lung: Tuberculosis (Caseous Necrosis)]] | |
| − | + | * [[IPLab:Lab 6:Tuberculosis|Lab 6: Lung: Tuberculosis]] | |
{{IPLab 3}} | {{IPLab 3}} | ||
[[Category: IPLab:Lab 3]] | [[Category: IPLab:Lab 3]] | ||
Latest revision as of 14:25, 25 August 2016
Contents
Clinical Summary[edit]
Two months prior to admission, this 57-year-old white male underwent a routine physical examination. During the course of the examination, a lesion was found in the upper lobe of the right lung. Initially, the patient was treated for two weeks with ampicillin. He was then admitted to the hospital for further study. All studies including sputum studies for tubercle bacilli, bronchial washings, and bronchoscopy were negative and he was discharged.
Upon re-admission, a review of systems revealed the presence of mild dyspnea on exertion, accompanied by a slightly productive cough. Of interest was the fact that the patient had had a positive PPD test for the past 4 to 5 years, but this had never been evaluated. At this time, physical and laboratory examinations were unremarkable. Radiographic examination of the chest revealed a 2 x 2-cm density in the right lower lung field. A CT scan revealed several small cavities in this area.
Findings[edit]
The patient underwent a thoracotomy, at which time a portion of the upper lobe of the right lung was removed. Examination of the cut surface revealed small white nodules measuring up to 0.2 cm in diameter.
Images[edit]

This is a gross photograph of a lung containing a nodular lesion at the lung apex (arrows). Note that the lesion appears solid and has a whitish coloration indicating considerable fibrous connective tissue. This is a healed granuloma due to primary tuberculosis in the lung. There are smaller focal lesions adjacent to the major mass. In addition, note the extensive anthracosis in this lung.
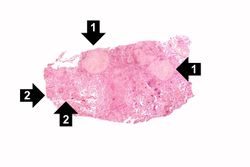
This low-power photomicrograph of a section of lung reveals multiple large nodules (1) with pale eosinophilic centers surrounded by a rim of blue-staining nuclei. In addition to the large nodules, there are several smaller nodules throughout the slide (2).
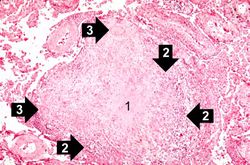
This is a photomicrograph of a tuberculosis granuloma. Note the central core of caseation necrosis (1) encircled by a rim of epithelioid macrophages and lymphocytes (2). Langhans’ type multinucleated giant cells are also present although they are difficult to see at this power (3).
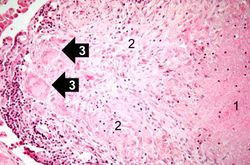
This is a high-power photomicrograph of a granuloma. Note the necrotic core on the right (1), epithelioid macrophages (2), and Langhans’ type giant cells (3) at the periphery of the granuloma. Note also the small lymphocytes characterized by their distinctly blue-staining nuclei. Other cells in the tissue, in addition to the macrophages, include fibroblasts and occasional neutrophils.
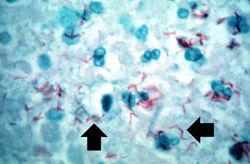
This high-power photomicrograph of a tuberculosis granuloma demonstrates acid-fast bacilli (arrows).





Virtual Microscopy[edit]
Lung: Tuberculosis H&E[edit]
Lung: Tuberculosis AFGT[edit]
Normal Lung[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Rodrigues DS, Medeiros EA, Weckx LY, Bonnez W, Salomão R, Kallas EG. Immunophenotypic characterization of peripheral T lymphocytes in Mycobacterium tuberculosis infection and disease. Clin Exp Immunol 2002 Apr;128(1):149-54.
- Horsburgh CR, Barry CE, Lange C. Treatment of Tuberculosis. NEJM 2015 Nov 26;373:2149-2160.
Images[edit]
Related IPLab Cases[edit]
Mycobateria grow very slowly on culture plates, with cultures requiring up to 6 weeks for a positive finding. In lieu of cultures, a more rapid diagnostic test is the PPD--purified protein derivative of tuberculosis--test. PPD is injected under the skin of an individual and then the area is reexamined in 48-72 hours for signs of an inflammatory reaction. A positive test indicates previous exposure to M. tuberculosis.
A thoracotomy is a surgical procedure in which an opening is made in the chest wall.
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.
A normal PaCO2 is 35 to 45 mmHg.
A normal partial thromboplastin time is 28 to 37 seconds.